@MissOrange Wow. You are looking good!!!Day 7 post full face fat graft and as I am finally deswelling I put on makeup today for my reveal. It took longer to deswell as I had had threads placed and removed. I was curious to see if my face lifted with fg alone. Here is my best shot...
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
How to go from 50+ to looking 20+ with plastic surgery rejuvenation.
- Thread starter MissOrange
- Start date
TPF may earn a commission from merchant affiliate
links, including eBay, Amazon, and others
- Status
- Not open for further replies.
More options
Who Replied?
Thanks @Fortunecat. I think to fit in better with the Brits I shall wear a curtain fringe to hide the round forehead. I bought Korean contact lenses Hologram brand in tear pearl sky gray and they make my eyes look naturally blue gray! Still managing to look 20s! It is now at a point where even I do not believe my real age.@MissOrange Wow. You are looking good!!!
Attachments



Last edited:
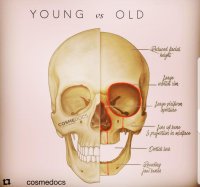
Today's post is on age related facial bone loss. As I turn 60 in 6.5 years it occurred to me that I may finally have a small face with age-related bone loss. But this suggests then that this may be the cause of extensive facial wrinkling and sagging in persons over 60 from excess loose skin with osteoporotic bone reduction, worse in small postmenopausal women than men whose bigger facial bones buy them time! The older facial bone photo looks like the after of a zygoma and v line facial contouring operation.
What happens to young persons who get these dramatic jaw reductions in their 20s when they reach 60? They won't have much bone left to support their teeth after 30%+ is lost with ageing? Does that mean they will need repeated fat grafts, threadlifts or smas FL to lift the loose saggy skin from bone reduction for the next 40 years? Do we see any 60 yo who has had dramatic facial contouring surgery in her 20s to see what happens? Will drastic FC surgery expedite ageing? Food for thought.
What happens to young persons who get these dramatic jaw reductions in their 20s when they reach 60? They won't have much bone left to support their teeth after 30%+ is lost with ageing? Does that mean they will need repeated fat grafts, threadlifts or smas FL to lift the loose saggy skin from bone reduction for the next 40 years? Do we see any 60 yo who has had dramatic facial contouring surgery in her 20s to see what happens? Will drastic FC surgery expedite ageing? Food for thought.
Attachments

Last edited:
Thanks @Fortunecat. I think to fit in better with the Brits I shall wear a curtain fringe to hide the round forehead. I bought Korean contact lenses Hologram brand in tear pearl sky gray and they make my eyes look naturally blue gray! Still managing to look 20s! It is now at a point where even I do not believe my real age.
You look absolutely adorable with the bangs! Love it (though your forehead is just fine imo)!
Thanks @yunggrandpa! I bet you look very young too based on your handle.You look absolutely adorable with the bangs! Love it (though your forehead is just fine imo)!
Thanks @yunggrandpa! I bet you look very young too based on your handle.
Aww, thank you! I'm just in my 20s though so I'll have to find out later on haha
 I must say though, it blows my mind how good you look - I could barely believe your age. Just amazing.
I must say though, it blows my mind how good you look - I could barely believe your age. Just amazing.you look amazing! wow, really great resultDay 7 post full face fat graft and as I am finally deswelling I put on makeup today for my reveal. It took longer to deswell as I had had threads placed and removed. I was curious to see if my face lifted with fg alone. Here is my best shot...
At 7 days you are still very swollen - favorable swelling from even a small amount of fat transfer lasts 3-6 months.
Today's post highlights the risks of plastic surgery in Korea as we read of yet another patient death. Sadly a 35 yo HK lady died during liposuction at a clinic near Sinsadong yesterday. https://www.google.co.uk/amp/m.koreatimes.co.kr/pages/article.amp.asp?newsIdx=282646
How can one die from liposuction? 1. If propofol iv is injected without access to a ventilator and the patient stops breathing like the late Michael Jackson. 2. With massive blood loss from extensive liposuction, the patient may go into cardiac arrest. 3. If combined with fat transfer, a pulmonary embolism may occur if fat is injected into a blood vessel.
The risk of surgery in an outpatient surgery clinic has been highlighted before with lack of resuscitation equipment or ventilator as one finds in a large hospital. The risk of larger hospitals is the use of shadow doctors or even dentists who may not even be board certified and may be paid a mere 500-700,000 krw per case.
With patient deaths, Korean fines realised have only been in the region of a mere 300,000 krw as death by negligence is not classified as murder in Korea nor is it recognised but instead the doctor may be charged with fraud, ie use of a shadow. http://www.newpolice.kr/news/articleView.html?idxno=106
Prices are cheaper in outpatient surgery clinics as often times iv sedation is administered by a nurse or doctor himself. If you are lucky you may get a qualified anaesthetist but with ratios of anaesthetist to doctor often 1:3 or more in small clinics, the one anaesthetist is usually sitting in on cases requiring general anaesthesia. In Korea it is common for mask general anaesthesia with nitrous oxide and oxygen which can be unpleasant to inhale before drifting to sleep. In the UK they use iv propofol then intubate while asleep so it is less unpleasant and the ratio of anaesthetist to surgeon is 1:1, ie every case, whether twilight iv or GA, has an attendant anaesthetist present at all times. In the UK and US, prep is done while the patient is asleep. In Korea I have been strapped to the theatre table awake and prepped with cold disinfectant over my face and body. This part is unpleasant and could be avoided if they put the patient to sleep first as in the UK.
There is also a difference in postop analgaesia. In Korea they do not give opiates like cocodamol or tramadol but only tylenol/paracetamol. You may wish to bring voltarol/diclofenac with you (swallow with milk to neutralise stomach acid and do mot take if you suffer from asthma or have a bleeding problem) when you fly to korea but narcotics like codeine are not permitted into korea. This means you may face agonising postop pain when recovering from rib cartilage extraction for rib rhino, extensive liposuction or even worse for bone facial contouring when on simple tylenol.
In Korea patients report intense throat pain after general anaesthesia like a knife cutting into their throat. This could be due to mucosal injury from forced intubation with the endotracheal tube, ie intubating roughly. In the US postop pain relief is adequate to provide analgaesia to cover any mucosal injury.
In cases of surgical complications, it may be nigh impossible to fly back to address the concern so the additional cost to fix in your own country should be taken into account in patients who fly overseas for plastic surgery.
For those who have never had general anaesthesia, there is a risk just like for young people running their first marathon, that a hereditary heart condition may be present and undiagnosed like IHSS or cardiomyopathy or valvular heart disease. Often times this is not picked up on ecgs and may require an echocardiogram or stress ecg test. Neither are done in korea as preop assessments and some may even forego a chest x ray and ecg in young patients. I would not recommend GA in Korea in a small clinic if it is your first time. Check with your family and relatived for any family history of heart problems.
Hope others can chime in their thoughts. For now I shall stick to plastic surgery in the UK or Belgium where I know I have a dedicated anaesthetist even for iv sedation. I think the wake up call was when I was asked to sign a consent form for iv propofol, midazolam and ketamine and told the doctor himself would administer and that there was no anaesthetist. It cost me my 400,000 krw deposit at a clinic near Sinsadong to cancel the surgery 10 minutes before I was scheduled for breast fat transfer but at least I did not risk my life unnecessarily.
How can one die from liposuction? 1. If propofol iv is injected without access to a ventilator and the patient stops breathing like the late Michael Jackson. 2. With massive blood loss from extensive liposuction, the patient may go into cardiac arrest. 3. If combined with fat transfer, a pulmonary embolism may occur if fat is injected into a blood vessel.
The risk of surgery in an outpatient surgery clinic has been highlighted before with lack of resuscitation equipment or ventilator as one finds in a large hospital. The risk of larger hospitals is the use of shadow doctors or even dentists who may not even be board certified and may be paid a mere 500-700,000 krw per case.
With patient deaths, Korean fines realised have only been in the region of a mere 300,000 krw as death by negligence is not classified as murder in Korea nor is it recognised but instead the doctor may be charged with fraud, ie use of a shadow. http://www.newpolice.kr/news/articleView.html?idxno=106
Prices are cheaper in outpatient surgery clinics as often times iv sedation is administered by a nurse or doctor himself. If you are lucky you may get a qualified anaesthetist but with ratios of anaesthetist to doctor often 1:3 or more in small clinics, the one anaesthetist is usually sitting in on cases requiring general anaesthesia. In Korea it is common for mask general anaesthesia with nitrous oxide and oxygen which can be unpleasant to inhale before drifting to sleep. In the UK they use iv propofol then intubate while asleep so it is less unpleasant and the ratio of anaesthetist to surgeon is 1:1, ie every case, whether twilight iv or GA, has an attendant anaesthetist present at all times. In the UK and US, prep is done while the patient is asleep. In Korea I have been strapped to the theatre table awake and prepped with cold disinfectant over my face and body. This part is unpleasant and could be avoided if they put the patient to sleep first as in the UK.
There is also a difference in postop analgaesia. In Korea they do not give opiates like cocodamol or tramadol but only tylenol/paracetamol. You may wish to bring voltarol/diclofenac with you (swallow with milk to neutralise stomach acid and do mot take if you suffer from asthma or have a bleeding problem) when you fly to korea but narcotics like codeine are not permitted into korea. This means you may face agonising postop pain when recovering from rib cartilage extraction for rib rhino, extensive liposuction or even worse for bone facial contouring when on simple tylenol.
In Korea patients report intense throat pain after general anaesthesia like a knife cutting into their throat. This could be due to mucosal injury from forced intubation with the endotracheal tube, ie intubating roughly. In the US postop pain relief is adequate to provide analgaesia to cover any mucosal injury.
In cases of surgical complications, it may be nigh impossible to fly back to address the concern so the additional cost to fix in your own country should be taken into account in patients who fly overseas for plastic surgery.
For those who have never had general anaesthesia, there is a risk just like for young people running their first marathon, that a hereditary heart condition may be present and undiagnosed like IHSS or cardiomyopathy or valvular heart disease. Often times this is not picked up on ecgs and may require an echocardiogram or stress ecg test. Neither are done in korea as preop assessments and some may even forego a chest x ray and ecg in young patients. I would not recommend GA in Korea in a small clinic if it is your first time. Check with your family and relatived for any family history of heart problems.
Hope others can chime in their thoughts. For now I shall stick to plastic surgery in the UK or Belgium where I know I have a dedicated anaesthetist even for iv sedation. I think the wake up call was when I was asked to sign a consent form for iv propofol, midazolam and ketamine and told the doctor himself would administer and that there was no anaesthetist. It cost me my 400,000 krw deposit at a clinic near Sinsadong to cancel the surgery 10 minutes before I was scheduled for breast fat transfer but at least I did not risk my life unnecessarily.
Attachments





Last edited:
@MissOrange
This lady who had FL with the Belgian had her ops in September 2017 and April 2018. She gave good reviews for both on RS.
On 26th June 2019 she says that, "I had a modified macs facelift 3months ago but still have bruising on my cheeks and bunching under the skin.. Will it go? Also when I speak my mouth pulls down to the side and it makes me look sad. It looks like the muscles haven't been lifted upwards. I had fat transfer to the face at the same time, also have pouches at the corners of my mouth which look strange. I'm really embarrassed and am aware of my family staring at me."
She could be referring to the same Belgian ops or a new FL a few months later. Either way it doesn't look good. Amongst the comment sections, there is talk that people are threatened if they leave negative reviews and people complaining that bad reviews disappear on there. Maybe trolls maybe not.
Have you met any ex patients in real life who have had FL with the Belgian that have lasted more than a year?
This lady who had FL with the Belgian had her ops in September 2017 and April 2018. She gave good reviews for both on RS.
On 26th June 2019 she says that, "I had a modified macs facelift 3months ago but still have bruising on my cheeks and bunching under the skin.. Will it go? Also when I speak my mouth pulls down to the side and it makes me look sad. It looks like the muscles haven't been lifted upwards. I had fat transfer to the face at the same time, also have pouches at the corners of my mouth which look strange. I'm really embarrassed and am aware of my family staring at me."
She could be referring to the same Belgian ops or a new FL a few months later. Either way it doesn't look good. Amongst the comment sections, there is talk that people are threatened if they leave negative reviews and people complaining that bad reviews disappear on there. Maybe trolls maybe not.
Have you met any ex patients in real life who have had FL with the Belgian that have lasted more than a year?
Attachments
Last edited:
Day 7 post full face fat graft and as I am finally deswelling I put on makeup today for my reveal. It took longer to deswell as I had had threads placed and removed. I was curious to see if my face lifted with fg alone. Here is my best shot...
ms orange I wonder where do you do your usual full face fg? Im considering to try. However I still have some QO filler left on my forehead and temples (5months old) do u think its ok to do fg at this moment?
@MissOrange I would like to get your advise wether I need a zygoma reduction or just tweak it by hidding it with fat. My friends told me I look better when my face has fat coz when i loose weight thats where it shows my big bony cheekbone. Here’s my xray for your reference. Sorry to bother u i just wanted to know your opinion

Today's post highlights the risks of plastic surgery in Korea as we read of yet another patient death. Sadly a 35 yo HK lady died during liposuction at a clinic near Sinsadong yesterday. https://www.google.co.uk/amp/m.koreatimes.co.kr/pages/article.amp.asp?newsIdx=282646
RIP. How tragic and eerie considering the timing of this given your own decision to pass on getting work done due to the anaesthesia practices of that clinic. I hope it comes out which clinic this was, while I know they have laws in Korea that suppress this information nothing is stopping a Chinese news source from reporting it right? If the clinic has been spread through word of mouth, please let me know.
Thank you for this. I shall try to postpone smas FL to age 60 if possible.@MissOrange
This lady who had FL with the Belgian had her ops in September 2017 and April 2018. She gave good reviews for both on RS.
On 26th June 2019 she says that, "I had a modified macs facelift 3months ago but still have bruising on my cheeks and bunching under the skin.. Will it go? Also when I speak my mouth pulls down to the side and it makes me look sad. It looks like the muscles haven't been lifted upwards. I had fat transfer to the face at the same time, also have pouches at the corners of my mouth which look strange. I'm really embarrassed and am aware of my family staring at me."
She could be referring to the same Belgian ops or a new FL a few months later. Either way it doesn't look good. Amongst the comment sections, there is talk that people are threatened if they leave negative reviews and people complaining that bad reviews disappear on there. Maybe trolls maybe not.
Have you met any ex patients in real life who have had FL with the Belgian that have lasted more than a year?
I had my last 2 full face fat grafts at MVP clinic with Dr HyoSeok Seo. He did my eyelid fg and upper bleph in 2016 and I tried his full face fg in 2018 with top up last month.ms orange I wonder where do you do your usual full face fg? Im considering to try. However I still have some QO filler left on my forehead and temples (5months old) do u think its ok to do fg at this moment?
- Status
- Not open for further replies.
Register on TPF! This sidebar then disappears and there are less ads!